7 Signs Celiac Disease Is Affecting Your Oral Health
Posted: Jul 5, 2020 in
Published July 2020 · Updated May 2026
Most people with celiac disease don’t find out from a stomach ache. They find out because their dentist notices something unusual — symmetrical grooves on their molars, enamel that’s eroding faster than normal, or gum tissue that won’t stop bleeding no matter how carefully they brush. Oral symptoms are often the first sign of celiac disease, appearing years before a gastroenterologist gets involved.
If you’ve been told your dental problems are “just genetics” and nothing else explains them, celiac disease may be worth investigating.
Table of Contents
- Why Celiac Disease Targets Your Mouth First
- The 7 Oral Signs of Celiac Disease
- Can Going Gluten-Free Reverse These Symptoms?
- Your Dentist May Spot Celiac Before Your Doctor Does
- Frequently Asked Questions
Why Celiac Disease Targets Your Mouth First
Celiac disease is not a gluten allergy — it’s an autoimmune disorder. Every time gluten enters the digestive system, the immune system mounts an attack that damages the lining of the small intestine. Over time, this impairs the absorption of key nutrients: calcium, vitamin D, iron, zinc, and B vitamins.
Your mouth bears the consequences. Calcium and vitamin D are essential for strong enamel and bone density. Iron and B vitamins support healthy gum tissue and saliva production. When absorption breaks down, every structure in your mouth becomes vulnerable — before you’ve had a single digestive symptom.
According to research published in the Journal of Gastroenterology and Hepatology, dental enamel defects are present in 40–75% of celiac patients — and in many cases, they’re what prompts the original diagnosis.
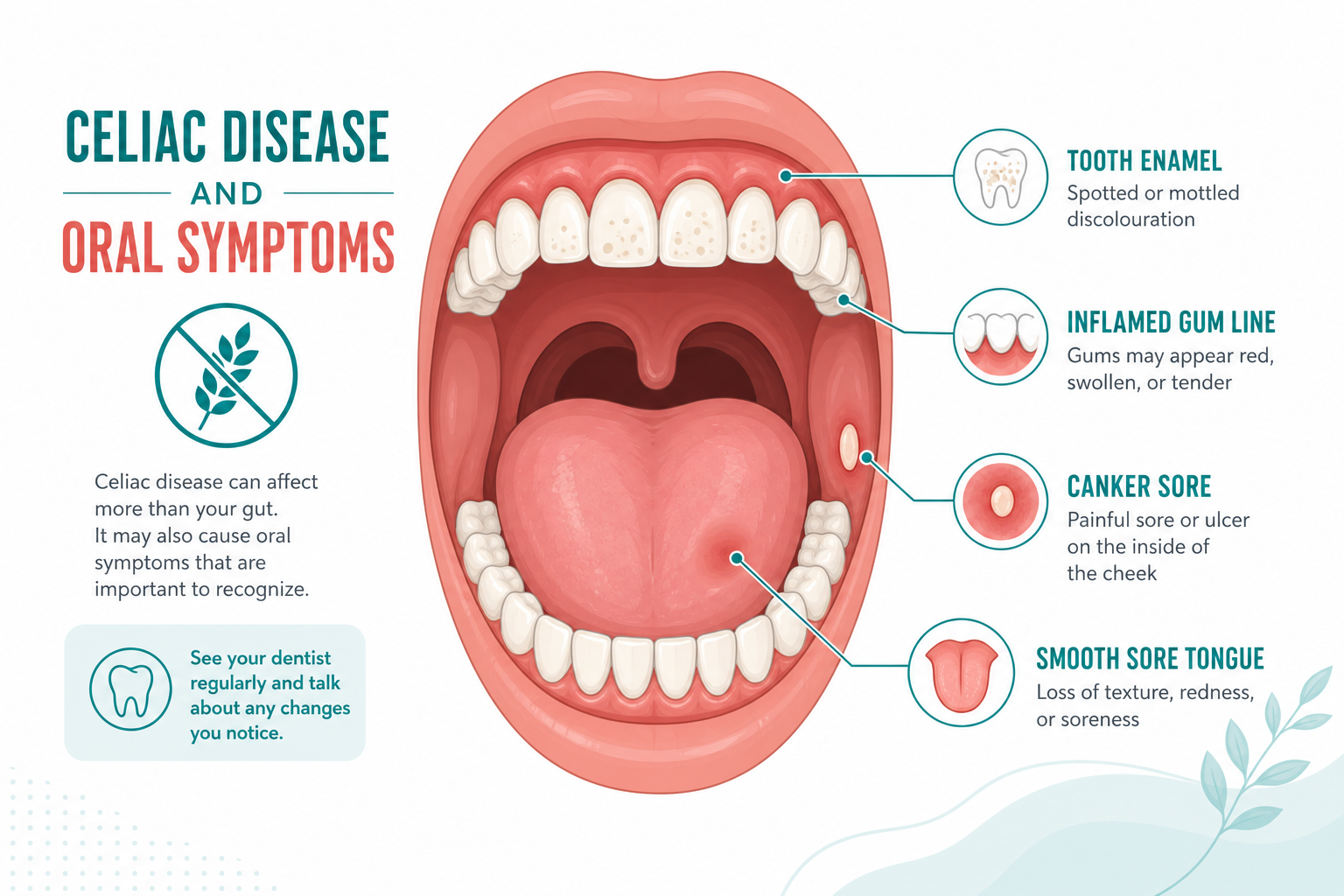
The 7 Oral Signs of Celiac Disease
These symptoms don’t all appear at once, and no single sign confirms celiac disease. But a pattern of several — especially the symmetrical ones — is a strong enough signal to mention to your dentist and follow up with your doctor.
1. Tooth Enamel Defects
This is the most diagnostically reliable oral sign. Celiac-related enamel defects are bilateral and symmetrical — meaning they appear in the same locations on both sides of the mouth, in a pattern that matches when the teeth developed. That symmetry is what separates celiac damage from damage caused by poor brushing or childhood illness.
Look for:
- White, yellow, or brown discolouration in bands or spots across multiple teeth
- Visible pits, grooves, or rough patches on the enamel surface
- Translucent or glassy-looking teeth where enamel has been lost entirely
These defects form during tooth development and cannot be undone — but they can be restored with bonding or veneers once the underlying condition is managed.
2. Chronic Canker Sores
Canker sores (recurrent aphthous stomatitis) are small, painful ulcers that form on the inside of the cheeks, lips, or base of the tongue. While most people get the occasional canker sore from stress or acidic food, people with untreated celiac disease tend to experience them more often, more severely, and with less obvious trigger.
The link is twofold: celiac disease dysregulates the immune system, which is believed to drive recurrent aphthous stomatitis; and nutritional deficiencies (particularly iron and B12) are a documented trigger. Studies have found that maintaining a strict gluten-free diet reduces canker sore frequency significantly in celiac patients.
3. Gum Disease and Gum Recession
Yes, celiac disease can cause gum recession. This surprises many patients because they’ve always been told gum disease is a brushing problem. And usually it is — but in people with celiac disease, the immune dysfunction adds a second pathway.
A healthy immune system manages the bacterial load in the mouth and limits gum inflammation. When that system is misfiring, the gums become chronically inflamed even with good oral hygiene. Research from the Celiac Disease Foundation found that 60% of children with untreated celiac disease showed clinical signs of gingivitis. In adults, this chronic inflammation — combined with calcium and vitamin D deficiency weakening the supporting bone — can progress to periodontitis and visible gum recession over time.
Signs to watch for: gums that bleed when you brush, gums that look swollen or pulled back from the teeth, or persistent gum sensitivity that doesn’t improve despite good home care.
4. Persistent Bad Breath
Celiac-related bad breath (halitosis) is not the kind that goes away with mouthwash. It comes from two sources that aren’t addressable at the surface level.
First: dry mouth (covered below) reduces saliva flow, allowing odour-causing bacteria to accumulate on the tongue, gumline, and between teeth without the natural rinsing saliva provides. Second: the digestive disruption from celiac disease itself — undigested food particles and bacterial imbalance in the gut — can produce volatile compounds that contribute to breath odour from the inside.
If you’ve been using breath mints and mouthwash without lasting improvement, and you also experience other symptoms on this list, the cause may be systemic rather than oral.
5. Dry Mouth
Saliva does far more than keep the mouth comfortable — it remineralises enamel, flushes bacteria, and buffers the acids produced by plaque. Celiac disease reduces salivary flow by impairing the absorption of the nutrients that support saliva gland function.
The downstream effects of dry mouth compound quickly:
- Tooth decay accelerates as acid stays in contact with enamel longer
- Gum disease risk increases as bacteria go unrinsed
- Canker sores and mouth sores develop as the tissue loses lubrication
- Bad breath worsens as bacterial load increases
Dry mouth that isn’t explained by medication side effects or another condition is worth investigating as a potential celiac symptom.
6. Delayed Tooth Eruption in Children
Celiac disease disrupts the development and eruption timeline for children’s teeth. The nutrient deficiencies it causes — particularly calcium and vitamin D — affect the mineralisation of teeth as they form, which can delay when they erupt and weaken their structure when they do.
General tooth development milestones to watch:
- A full set of 20 baby teeth by age 3
- First baby teeth falling out around age 6, continuing over 4–6 years
- A complete set of 28 permanent teeth by age 12–13
If your child’s teeth are erupting significantly later than these benchmarks — or if their teeth show the enamel defects described above — mention celiac disease to their dentist and paediatrician.
7. Atrophic Glossitis (Smooth, Sore Tongue)
The tongue is normally covered in small bumps called papillae. Atrophic glossitis — a well-documented celiac symptom — causes these papillae to flatten or disappear entirely, leaving the tongue looking unusually smooth, shiny, or “bald.”
The condition is caused by deficiencies in iron, B12, and folate — all nutrients that celiac disease prevents the body from absorbing adequately. Alongside the change in appearance, the tongue may feel sore, tender, or burning, especially when eating acidic or spicy foods.
Can Going Gluten-Free Reverse These Symptoms?
For most oral symptoms: yes, but it takes time. Eliminating gluten stops the autoimmune reaction, allows the intestinal lining to heal, and gradually restores normal nutrient absorption. As nutritional status improves, many patients see measurable changes in their oral health within 12–24 months:
- Canker sore frequency decreases — often the first symptom to improve
- Gum inflammation reduces and bleeding on brushing lessens
- Dry mouth improves as salivary function recovers
- Bad breath resolves once the bacterial imbalance corrects itself
The one exception is tooth enamel defects — enamel that has already formed with defects cannot repair itself. Those require cosmetic dental treatment (bonding, veneers, or composite restoration) after the systemic issue is under control.
Your Dentist May Spot Celiac Before Your Doctor Does
This isn’t hypothetical — it’s documented. Because dental enamel defects from celiac disease follow a specific bilateral, symmetrical pattern that differs from decay or injury, a trained eye can identify the signature during a routine examination.
At Woodcreek Dental Care, when we see a pattern of symmetrical enamel defects combined with recurrent canker sores, chronic gum inflammation that doesn’t respond to cleaning, or atrophic glossitis, we discuss the possibility of celiac disease with the patient and recommend they follow up with their physician for a blood test (anti-tTG IgA) or referral to a gastroenterologist.
If you’ve had persistent unexplained dental problems and have never been tested for celiac disease, a comprehensive dental exam is a reasonable place to start.
Book a Dental Exam at Woodcreek →
Frequently Asked Questions
Can celiac disease cause gum recession?
Yes. Celiac disease contributes to gum recession through two mechanisms: the autoimmune dysfunction chronically inflames gum tissue even with good oral hygiene, and the nutrient deficiencies it causes (calcium, vitamin D) weaken the supporting jaw bone over time. Patients with untreated celiac disease have significantly higher rates of gingivitis and periodontitis than the general population.
Can celiac disease cause bad breath?
Yes. The most common mechanism is dry mouth — celiac disease impairs absorption of nutrients needed for saliva production, reducing salivary flow and allowing odour-causing bacteria to multiply. A second pathway is digestive: the bacterial imbalance caused by celiac disease in the gut can produce volatile compounds that contribute to breath odour. Standard mouthwash does not resolve celiac-related halitosis.
Does celiac disease affect tooth enamel?
Yes, and this is one of the most clinically specific signs. Celiac-related enamel defects are bilateral and symmetrical — they appear in matching locations on both sides of the mouth, reflecting the timing of tooth development when nutrient absorption was disrupted. They cannot be reversed, but they can be restored cosmetically once the underlying condition is managed.
Can a dentist detect celiac disease?
Dentists cannot diagnose celiac disease, but they can identify the oral patterns that make it worth investigating — particularly the bilateral enamel defects and chronic gum inflammation that don’t respond to standard treatment. A dentist may refer you to your GP for a blood test (anti-tTG IgA) or gastroenterology consultation.
Does going gluten-free improve dental symptoms?
Yes, for most symptoms other than existing enamel defects. Canker sore frequency, gum inflammation, dry mouth, and bad breath typically improve within 12–24 months of a strict gluten-free diet as nutritional absorption is restored. Enamel that has already formed with defects requires cosmetic dental treatment to correct.
Sources: Dental and Oral Manifestations of Celiac Disease — NCBI · Oral Health — Celiac Disease Foundation · Canadian Celiac Association
About the author: The clinical team at Woodcreek Dental Care has provided family and general dentistry to SW Calgary for over 30 years.